The California Department of Public Health has just released a report that detailed the number of terminally ill patients over the past year who took advantage of the California End-of-Life Options Act (EOLA), a law that allows certain patients to request a lethal dose of medication to end their lives. This report comes a year after EOLA went into effect on June 9, 2016.
According to the report, 258 individuals began the end-of-life process, which requires multiple oral and written requests and discussions with doctors before receiving the medication. Of this group, 90 patients received a prescription to end life but did not take it, while 111 individuals died from ingesting the drugs.
Supporters believe aid-in-dying laws are important for terminal patients because they provide an option to end life on their terms, rather than in a hospital or hospice setting. Indeed, there is a growing consensus in the United States in favor of aid-in-dying. According to a May 2017 Gallup Poll, 73 percent of US adults surveyed believe a doctor should be allowed to help a terminally ill patient end his or her life if the patient makes the request. Six states and the District of Columbia permit aid-in-dying, and more states are considering similar laws.
One critical question is whether these laws make the process accessible to everyone who wants this option.
I am a sociologist who studies aid-in-dying laws and how law influences end-of-life choice. People often ask: Who is the typical person who pursues this option? My research looks at this question with data I combined from California along with Oregon and Washington, states that have published information about the people who use aid-in-dying laws.
A Fairly Homogeneous Group
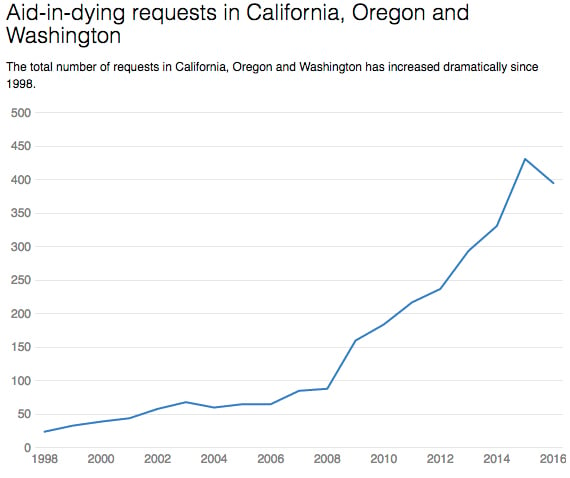
In California, 258 people began the end-of-life process between June 2016 and June 2017, lower than the 431 requests in 2015 in Oregon and Washington combined. California’s EOLA may ultimately result in more requests, given the state’s large population.
 Data from California Department of Public Health, Oregon Health Authority and Washington State Department of Health. The Conversation, CC-BY-ND.
Data from California Department of Public Health, Oregon Health Authority and Washington State Department of Health. The Conversation, CC-BY-ND.
The numbers we have — predominantly based on Oregon and Washington patients — indicate that aid-in-dying patients are more likely to be male, white, over 65 years old and with the minimum of a bachelor’s degree.
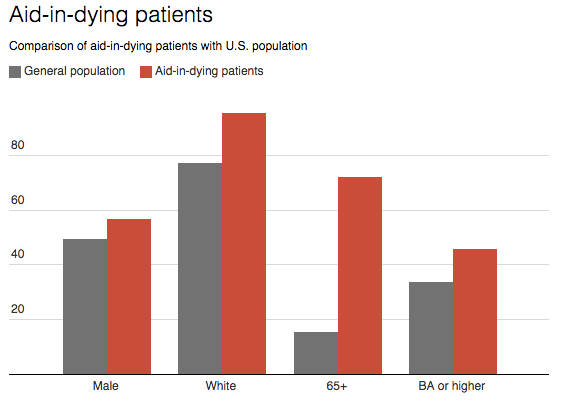 Data obtained from US Census, Oregon Health Authority, Washington State Department of Health and California Department of Public Health. The Conversation, CC-BY-ND.
Data obtained from US Census, Oregon Health Authority, Washington State Department of Health and California Department of Public Health. The Conversation, CC-BY-ND.
Why is a fairly homogeneous population using these laws more than others?
There may be many factors why these older white men are overrepresented, including access to doctors willing to help, religious beliefs or having peers with similar attitudes about aid-in-dying.
It is important, however, to also consider other explanations that may restrict access for certain populations.
Physicians are not required to help a patient who requests end-of-life options. New research shows that doctors struggle with professional and personal ethics around helping terminally ill patients and whether they should be required to inform patients who may not know about these laws.
Also, studies suggest racial differences about end-of-life choices are both cultural and structural. Pew Research Center shows African-Americans and Latinos are more religious, which includes belief in God, church attendance and prayer. Virtually all religions condemn aid-in-dying except the Unitarian Universalist Church. Religiosity explains a possible correlation between race and attitudes concerning aid-in-dying.
However, studies also report racial disparities with end-of-life care can be explained by the high cost of health care, lack of awareness regarding end-of-life care options, language barriers and high levels of distrust in medical professionals.
The growing number of aid-in-dying laws in more racially diverse states may change these trends. California is more diverse than other states, so it will be a state to watch in the years to come.
Barriers in Life and in Death
As more states consider aid-in-dying laws and discussions around end-of-life options are growing, it is important to question the statistics and what they do and don’t reveal.
Statistics about aid-in-dying provide transparency concerning a process where patients are given an option over their end-of-life plans. Statistics also reveal that not everyone who pursues aid-in-dying actually takes the medication. In fact, 42 percent of patients who received medication did not ingest it.
Some organizations are advocating on behalf of patients who would like to end their lives. Organizations such as Compassion & Choices and the Coalition of Compassionate Care of California work to bridge the gap between patients and providers by offering presentations to doctors and directories of medical professionals willing to help patients who choose this route.
The statistics are important to help identify patterns that may be the result not simply of different attitudes about end-of-life options, but rather structural barriers that keep certain groups from pursuing options at life’s end.
![]()
![]()
Join us in defending the truth before it’s too late
The future of independent journalism is uncertain, and the consequences of losing it are too grave to ignore. We have hours left to raise the $12,0000 still needed to ensure Truthout remains safe, strong, and free. Every dollar raised goes directly toward the costs of producing news you can trust.
Please give what you can — because by supporting us with a tax-deductible donation, you’re not just preserving a source of news, you’re helping to safeguard what’s left of our democracy.